
Getting pregnant with an IUD is rare, but it does happen.
Research puts the annual failure rate below 1%, yet the circumstances that raise that risk are rarely explained clearly.
This blog breaks down exactly what the odds look like, why failures happen, and what to do if you think yours might have.
How effective is an IUD?
IUDs are among the most reliable contraceptive methods available, more effective than the pill, the patch, or the implant in most real-world comparisons.
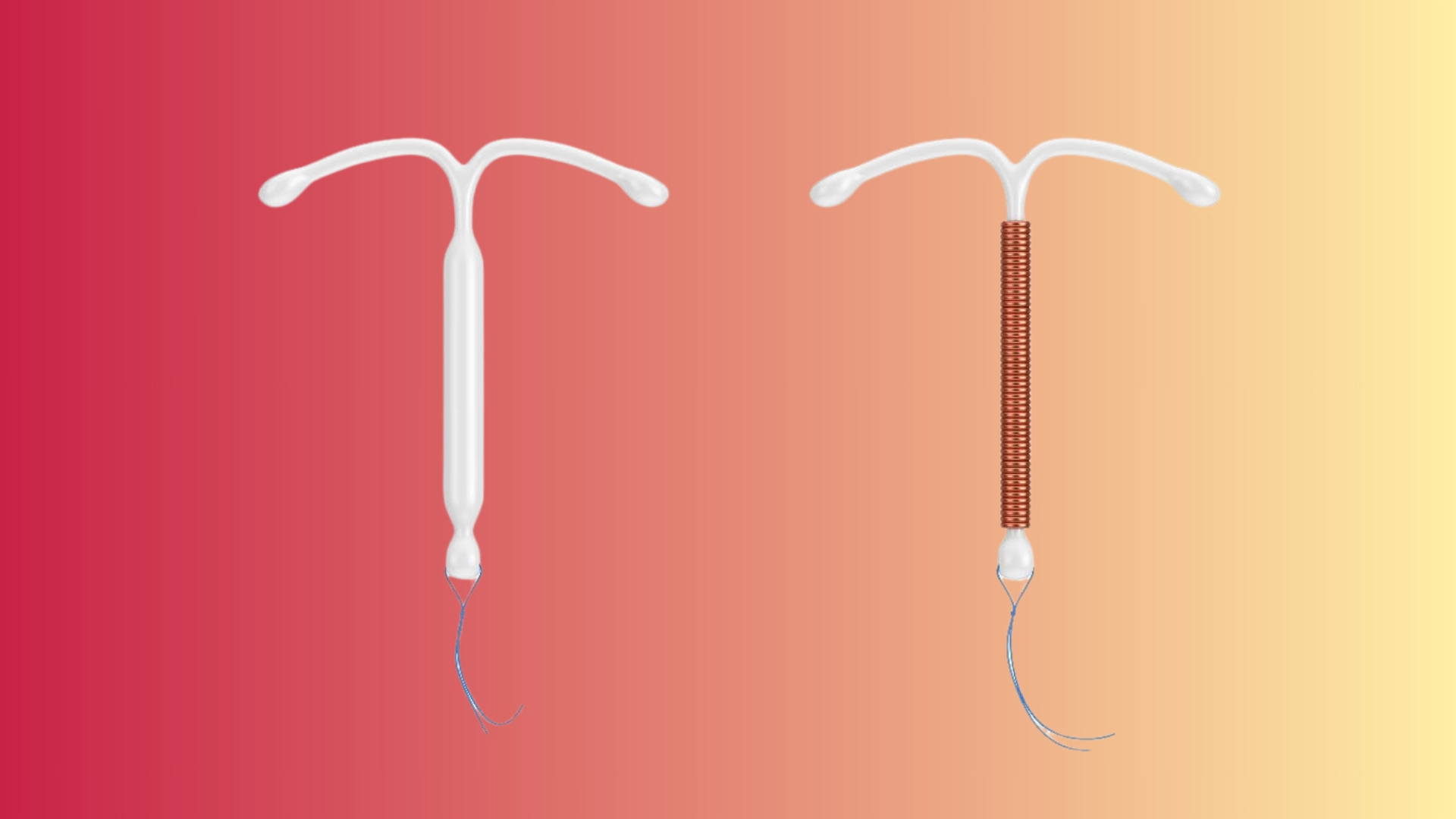
Hormonal IUDs like Mirena sit at over 99.8% effectiveness. The copper IUD is close behind, at around 99.2%.
These aren’t manufacturer claims; they’re figures drawn from large clinical trials and referenced in the ACOG and the RCOG guidance.
The reason they perform so well is partly the method itself and partly the absence of user error. Nothing to remember daily and nothing that interacts with a missed dose.
That said, effectiveness isn’t absolute.
Correct placement is also very important. So does timing, particularly with the copper IUD used as emergency contraception.
IUD effectiveness compares to other birth controls
A contraceptive method means weighing more than just convenience.
Effectiveness data, particularly the gap between perfect use and typical use, tells a more honest story.
| Contraceptive Method | Perfect Use | Typical Use |
|---|---|---|
| Hormonal IUD (Mirena/Kyleena) | 99.8% | 99.8% |
| Copper IUD | 99.2% | 99.2% |
| Combined Pill | 99.7% | 91% |
| Progestogen-Only Pill | 99.7% | 91% |
| Male Condom | 98% | 85% |
| Contraceptive Implant | 99.9% | 99.9% |
| Contraceptive Injection | 99.8% | 94% |
| Diaphragm | 94% | 88% |
IUDs and implants show no gap between perfect and typical use, because there’s no user action required after insertion.
Chances of getting pregnant with an IUD
IUDs are over 99% effective, meaning fewer than 1 in 100 people will conceive in a given year. Still, understanding what affects that number is important.
Pregnancy rates for hormonal IUDs
Hormonal IUDs– Mirena, Kyleena, and Liletta suppress ovulation and thicken cervical mucus, making fertilization unlikely.
Failure rates range from 0.1% to 0.2% annually in clinical trial data. That’s roughly 1 in 500 to 1 in 1,000 users per year.
Effective, but not infallible.
Pregnancy rates for copper IUDs
Copper IUD works differently: no hormones, just copper ions that are toxic to sperm. Annual failure rates land around 0.6% to 0.8%.
Slightly higher than hormonal options, but still more reliable than most other non-surgical methods available.
Why do pregnancies sometimes happen despite an IUD?
An IUD is highly reliable, but pregnancies do still occur in rare cases. A few specific reasons explain why this happens.
1. IUD expulsion
IUDs can partially or fully expel or dislodge from the uterus without the person realizing.
It happens in roughly 2–10% of users, most commonly in the first year.
When that happens, contraceptive protection drops significantly. Checking the strings monthly is the simplest way to catch it early.
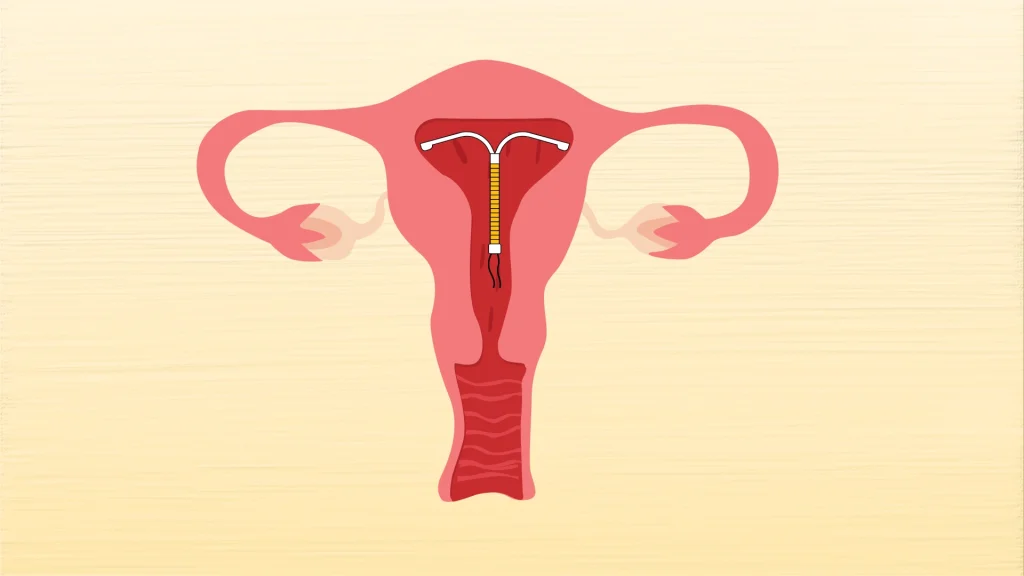
2. Incorrect IUD placement
Placement is very important, more than most people are told.
An IUD inserted even slightly off-position in the uterine cavity can fail to prevent pregnancy.
In clinical settings, this is typically caught during a follow-up ultrasound, but not everyone gets one routinely. If there’s any doubt after fitting, it’s worth asking for imaging.
3. Using an IUD beyond its recommended lifespan
Every IUD has a licensed duration, five years for some hormonal types, up to ten years for the copper IUD.
Using one beyond that window isn’t inherently dangerous, but data on its effectiveness beyond the licensed period is limited.
The straightforward advice: replace it on schedule and don’t assume it’s still working at full capacity.
4. Becoming pregnant before the IUD takes full effect
Hormonal IUDs inserted outside the first seven days of a menstrual cycle may not provide immediate protection.
The copper IUD is effective from insertion.
Assuming full protection from day one, regardless of cycle timing, is one of the more common and easily avoided sources of unintended pregnancy post-insertion.
5. Anatomical changes that affect IUD positioning
Uterine anatomy isn’t static.
Fibroids, a retroverted uterus, or changes following pregnancy can all shift how an IUD sits over time.
These aren’t rare edge cases; they’re factors that arise regularly in reproductive health clinics and can quietly affect how well the device performs its job.
Types of pregnancy with an IUD
The type of pregnancy that occurs with an IUD in place matters clinically, not just statistically. Two distinct scenarios can unfold, each carrying very different risks and management pathways.
Intrauterine pregnancy
An intrauterine pregnancy with an IUD in situ, meaning the embryo implants inside the uterus, is the more common of the two scenarios.
It still carries elevated risks compared to a standard pregnancy, including miscarriage and preterm labor.
In clinical settings, the IUD is usually removed as early as safely possible to reduce those risks.
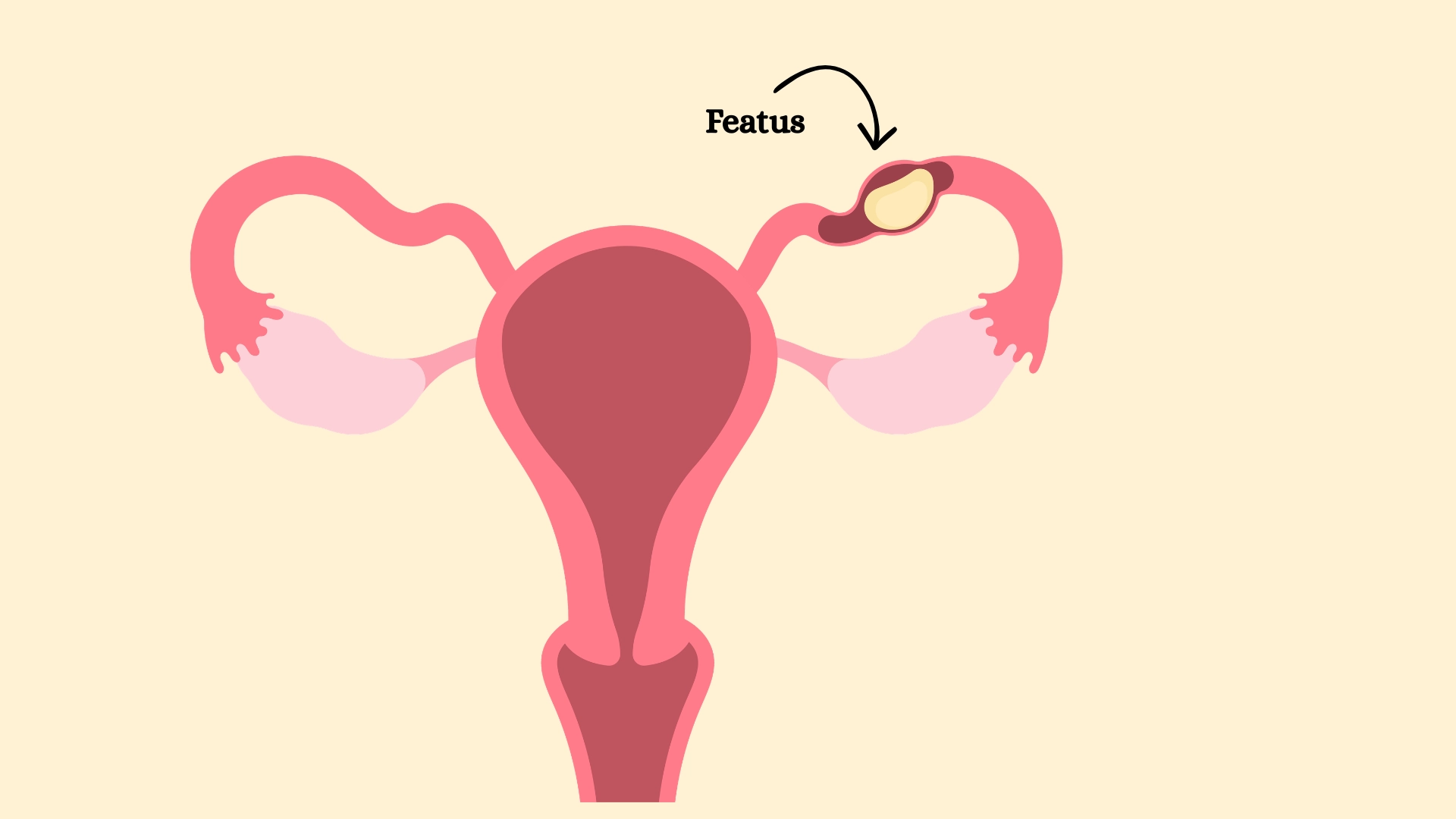
Ectopic pregnancy
An ectopic pregnancy occurs when a fertilized egg implants outside the uterus, most often in a fallopian tube.
IUDs don’t cause ectopic pregnancies, but if pregnancy does occur with one in place, the relative likelihood of it being ectopic is higher than in the general population.
It’s a medical emergency. Symptoms include one-sided pelvic pain, shoulder tip pain, and unusual bleeding.
If you suspect an ectopic needs a same-day medical assessment, not a wait-and-see approach.
Signs of pregnancy with an IUD
Pregnancy symptoms with an IUD in place aren’t always obvious, and some overlap with normal hormonal side effects of the device itself.
Knowing what to look for and when to act on it matters.
1. Missed or unusually light periods
Hormonal IUDs often lighten periods naturally, which makes a missed period harder to read.
Any unexpected change in the menstrual cycle pattern, particularly when accompanied by other symptoms, warrants a pregnancy test.
2. Nausea and morning sickness
Nausea that occurs without an obvious cause, especially in the morning, is one of the earliest signs of pregnancy.
It doesn’t always mean vomiting. Persistent queasiness alone is enough reason to test.
3. Breast tenderness and swelling
Breast tenderness can signal hormonal shifts linked to early pregnancy.
If it feels different from usual premenstrual soreness, more intense and longer-lasting, it’s worth paying attention to rather than dismissing.
4. Increased fatigue and sleepiness
Unusual, unexplained exhaustion in early pregnancy is driven by rising progesterone levels.
In clinical settings, patients often describe it as a heaviness that sleep doesn’t fully resolve, distinct from ordinary tiredness.
5. Frequent urination
Needing to urinate more often than usual, without a change in fluid intake or signs of infection, can be an early pregnancy indicator.
It typically appears within the first few weeks of implantation.
6. Cramping or pelvic discomfort
Cramping with an IUD in place isn’t automatically concerning.
But cramping that feels one-sided, sharp, or different from usual, particularly with a missed period, needs same-day medical attention to rule out ectopic pregnancy.
Does the age of the IUD play a role in pregnancy?
Yes, and it’s a factor that doesn’t always get enough attention.
Every IUD has a licensed effective lifespan, and staying within that window matters.
Hormonal IUDs typically last between three and eight years, depending on the brand. The copper IUD is licensed for up to ten years.
As an IUD approaches or exceeds that timeframe, hormone levels in hormonal devices drop, and copper ion release in non-hormonal ones may reduce.
Both scenarios mean reduced contraceptive efficacy.
The evidence beyond licensed durations is limited, which is itself the problem. There isn’t enough robust trial data to confidently say an expired IUD still works.
Replacing it on schedule isn’t overcautious. It’s the clinically sound decision.
Risks associated with getting pregnant with an IUD
Pregnancy with an IUD in place isn’t just statistically unlikely; it also carries specific clinical risks that make early detection and prompt medical attention important.
These aren’t worst-case scenarios. They’re documented outcomes that inform how this situation is managed.
1. Increased risk of ectopic pregnancy
If pregnancy occurs with an IUD in place, the chance of it being ectopic, implanting outside the uterus, is disproportionately higher than in unassisted pregnancies.
This isn’t because IUDs cause ectopic pregnancies. It’s because they’re more effective at preventing intrauterine implantation.
One-sided pelvic pain and unusual bleeding warrant same-day assessment.
2. Risk of infection and pregnancy complications
An IUD string passing through the cervix creates a potential pathway for bacterial migration during pregnancy.
This raises the risk of intrauterine infection, chorioamnionitis, which can affect both the pregnancy and longer-term fertility.
In reproductive health clinics, this is one of the primary reasons early removal is recommended when an intrauterine pregnancy is confirmed.
3. Miscarriage and preterm birth concerns
Continuing a pregnancy with an IUD in situ significantly raises miscarriage risk, particularly in the second trimester. Preterm labor is also more likely.
The data here is consistent across multiple studies, though exact figures vary by IUD type and gestational timing of detection.
Early removal, where strings are accessible, reduces but doesn’t eliminate these risks.
4. Risks of leaving the IUD in place during pregnancy
Removing an IUD early in pregnancy carries some risk. Leaving it in carries more.
If strings aren’t visible or accessible, removal becomes technically difficult, and in those cases, the decision involves careful clinical judgment rather than a straightforward protocol.
Anyone in this situation needs specialist input, not general reassurance.
Steps to take if you are pregnant
Suspecting a pregnancy with an IUD in place calls for quick, clear action, not panic, but not delay either. The steps below outline exactly what needs to happen and why the order matters.
Take a home pregnancy test
A standard urine pregnancy test detects hCG, human chorionic gonadotropin, the hormone produced after implantation.
They’re reliable from the first day of a missed period.
A positive result with an IUD in place means one thing: contact a healthcare provider the same day, not after the weekend.
Contact your healthcare provider
This isn’t a situation that warrants waiting for a routine appointment.
A pregnancy with an IUD in situ needs prompt clinical assessment, ideally within 24 hours of a positive test.
In reproductive health clinics, this kind of presentation is treated as time-sensitive. Call ahead, explain the situation clearly, and ask for an urgent slot.
Confirm the pregnancy
A home test is a starting point, not a diagnosis.
Blood hCG levels and an early ultrasound are needed to confirm the pregnancy, establish gestational age, and, critically, determine where implantation has occurred.
This step isn’t optional. It’s the information that shapes every clinical decision that follows.
Determining whether the pregnancy is ectopic
Ruling out an ectopic pregnancy is the most urgent clinical priority at this stage.
A transvaginal ultrasound, where a small probe is used to visualize the uterus and fallopian tubes directly, is the standard first step.
Symptoms like one-sided pelvic pain, shoulder tip pain, or unusual bleeding before confirmation should prompt emergency attendance, not a scheduled appointment.
If you are not pregnant, here are tips to prevent it
Lowering the already small risk of IUD failure comes down to a few consistent habits.
None of them are complicated, but skipping them is where preventable problems tend to start.
- Checking IUD strings correctly: Check monthly, after each period, by reaching for two thin strings just inside the cervix. If they feel shorter, longer, or absent, seek assessment promptly.
- Attending recommended follow-up visits: A check-up three to six weeks post-insertion confirms correct placement. Don’t skip it; this is when positioning problems are most likely to be caught.
- Knowing when your IUD needs replacement: Every IUD has a licensed lifespan. Track the insertion date and replacement window. Assuming it’s still working past its expiry isn’t a safe bet.
- Warning signs that the device may have moved: Cramping outside a normal cycle, a partner feeling the strings during sex, or strings that feel different are all reasons to get checked sooner rather than later.
To wrap it
IUDs are reliable, but no contraceptive method is completely without risk.
Incorrect placement, expulsion, timing, and aging of the device are all factors that quietly affect how well an IUD performs.
The risks associated with an IUD pregnancy, ectopic implantation, infection, and miscarriage are serious enough that early detection is crucial.
If something feels off- unusual cramping, a missed period, strings that don’t feel right- get checked. Not next week.
That’s the practical takeaway from everything covered here.
If you are weighing contraceptive options, speaking with a reproductive health specialist is always the right next step.
People may ask
1. Will I test positive if pregnant with an IUD?
Yes. A home pregnancy test detects hCG regardless of the contraception used. A positive result means seeking a same-day medical assessment.
2. Can sperm go around an IUD?
An IUD doesn’t physically block sperm. It prevents pregnancy through hormonal effects or copper ions, not as a barrier.
3. What is the 5 3 1 rule in pregnancy?
This refers to contraction timing in labor, five minutes apart, lasting thirty seconds, for one hour. Unrelated to IUD use.




